Hi Zach,
Welcome to the Meteor forums. Great insights; great comments.
So, yes… not to put too fine a point on it, but HL7 FHIR stands to drop the bottom out of the integration services market.
My experience has been that HL7 integration is usually something like a $5,000 line-item on systems installation. Buy a digital microscope; centrifuge; ultrasound scanner; voice recognition system; whatever… somewhere in the bill will be a $5K installation fee for HL7 point-to-point bidirectional interface. At the hospital I used to work at, we had 30 interfaces when I began; and probably 50 when I ended. It was enough to keep a few people employed full-time just doing HL7 interface work (and on-call).
With HL7 FHIR, however, we have a RESTful interface with one-to-many connections. So, we’re anticipating there to be a $5K to $10K installation fee to set up a FHIR server (depending on LDAP integration; hardware installation etc.) with something like a $1,000 fee per resource (which will mostly involve writing a SQL query at the ORM layer). If a hospital wants to implement all 100 resources, that will still keep one of those HL7 analysts busy for most of a year; but once each resource is mapped, the analyst will have effectively finished the job and can move onto other projects. In effect, it’s a write-once, read-as-much-as-you-like interface.
Device vendors should be able to get interoperability for $15,000 or so, since they’ll only have a few (3 to 5) resources to implement.
Once a lot of the initial mapping is completed, it should be a paltry $250 to write the AJAX to connect to a pre-existing FHIR server; and we’ll see bidirectional connectivity for as low as $500. Which matches your factor of 10x.
As the price drops, the entire interconnectivity market is going to become much more liquid, and folks will begin bypassing the hubs; and things will become much more mesh-like. Personally, I anticipate peer-to-peer applications following a WordPress model to become a trend in the consumer market in about 2 years.
As for testing, take a look at both Project Crucible and the Touchstone Project. Most all of the big players are on board with FHIR. So while the hubs, integrators, and exchanges based on V2 aren’t going to be happy that their billable hours are drying up; they all knew that it was stimulus money from HITECH. They’re simply going to have to get more competitive. The EMR vendors however… their main sources of revenue isn’t in HL7 integration services, so they could care less. It helps them to be more accessible, and people are demanding it.
But what I’m really excited about is that HL7 FHIR resources work perfectly well on the database. This doesn’t apply to SQL/Oracle systems; but for JSON datastore like Mongo, we can go from wire-to-database and database-to-wire with no ORM mapping layer. Meaning the FHIR resources are perfectly viable as database schemas, not just wire transfer formats. That means we can seemlessly connect applications to the same Mongo collections as long as the applications use the same FHIR resources. In effect, the HL7 standards committee provided a database spec for writing our own EMR apps and got the big vendors to agree to be compatible. So, we think we can induce demand for HL7 FHIR by simply writing FHIR compliant apps.
As far as funding goes, I just bundle HL7 into consulting arrangements. I’ve yet to meet a company that doesn’t want HL7 connectivity; and FHIR gives an easy standard to rally stakeholders around. Instead of having inane conversations about “Should we call it a Company or an Organization or an Entity?’” you can just point to FHIR and say, “Here’s the schema for an Organization; lets get to work.” And everybody is happy to get on board, because they want to be doing crazy advanced stuff like medication reconciliation or 3D stereotactic surgery or pharmacy robots or genome sequencing… not debating ontologies.
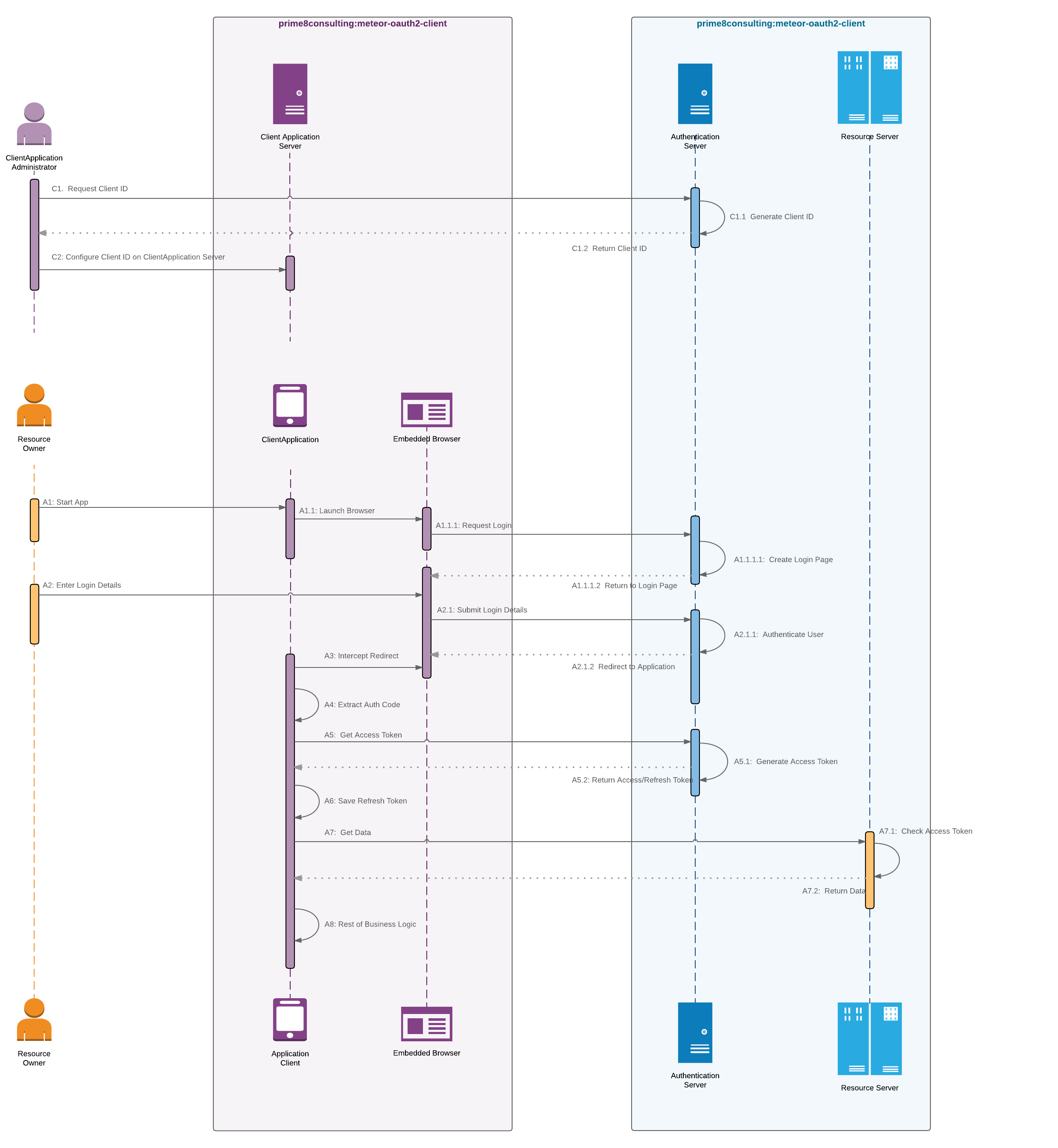
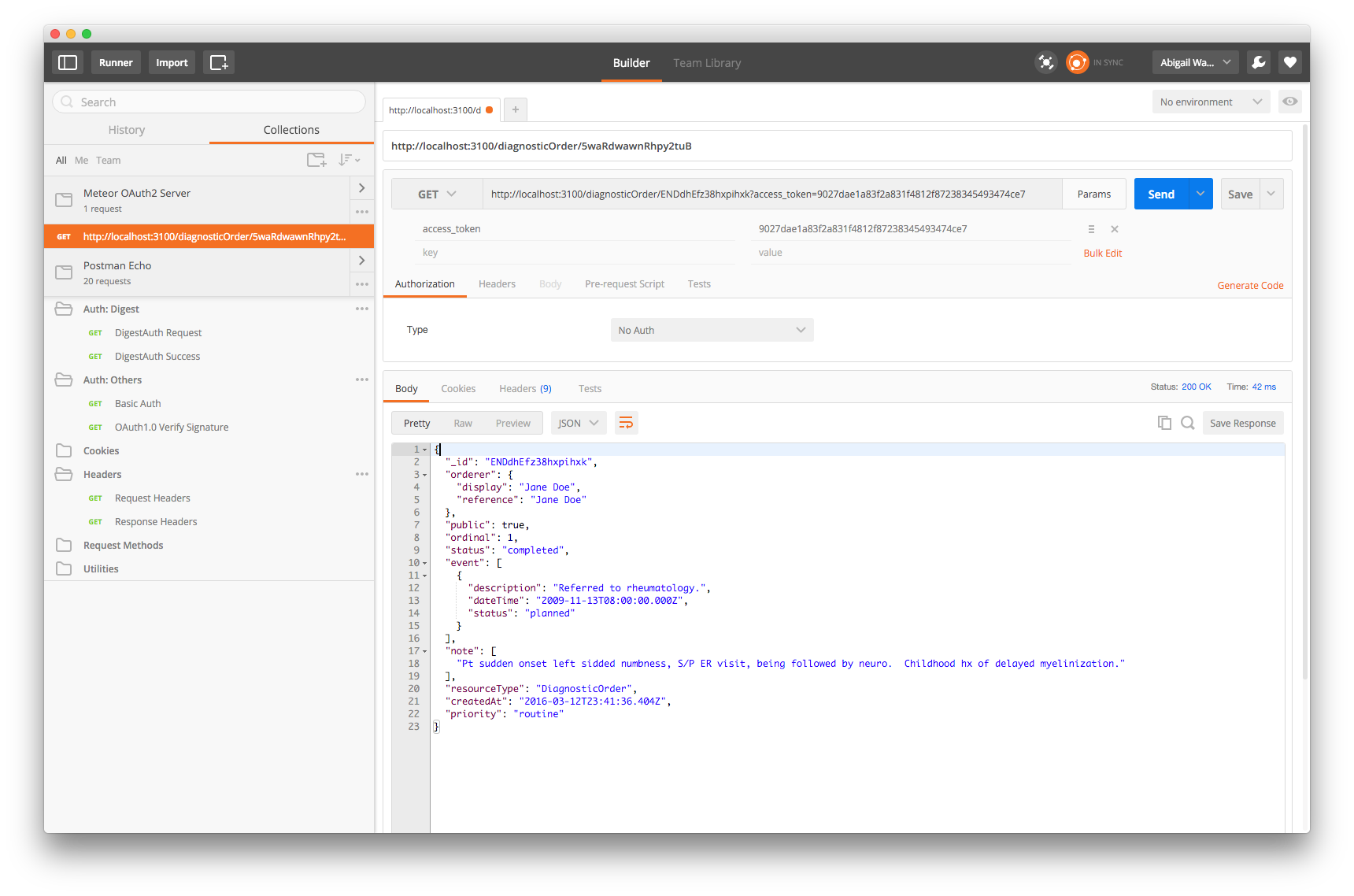
Anyhow, we’ve just about got the FHIR server all set up… we have the OAuth server, the REST API, and the FHIR resource schemas. Now we just have to put it all together. And then connect a sample app to query the server. Plenty of opportunity to participate and contribute.
Best,
Abigail

 ). But, a new highly-efficient protocol could be smothered in the lab-EMR space unless you can find a way to align with or work-around these ‘hubs.’ For many of these companies, this is a threat to replace their business model as they typically charge a flat fee for every single HL7 connection created to an EMR, so it may be tough to get them onboard if you’re providing a more efficient way to do things and replacing their billable hours… It would be possible to work around them if leveraging the protocol requires very little manual labor on the lab’s part and if you can automatically distribute the update to the lab’s EMR/LIS installation, e.g. allowing the labs to use the new protocol without the hub’s intervention… We don’t charge per connection (our model is unlimited connections for $x/month), so we’re more than happy to align with something more efficient.
). But, a new highly-efficient protocol could be smothered in the lab-EMR space unless you can find a way to align with or work-around these ‘hubs.’ For many of these companies, this is a threat to replace their business model as they typically charge a flat fee for every single HL7 connection created to an EMR, so it may be tough to get them onboard if you’re providing a more efficient way to do things and replacing their billable hours… It would be possible to work around them if leveraging the protocol requires very little manual labor on the lab’s part and if you can automatically distribute the update to the lab’s EMR/LIS installation, e.g. allowing the labs to use the new protocol without the hub’s intervention… We don’t charge per connection (our model is unlimited connections for $x/month), so we’re more than happy to align with something more efficient. Do these points resonate with your experiences? Are we approaching the same problem?
Do these points resonate with your experiences? Are we approaching the same problem?